|
What's New
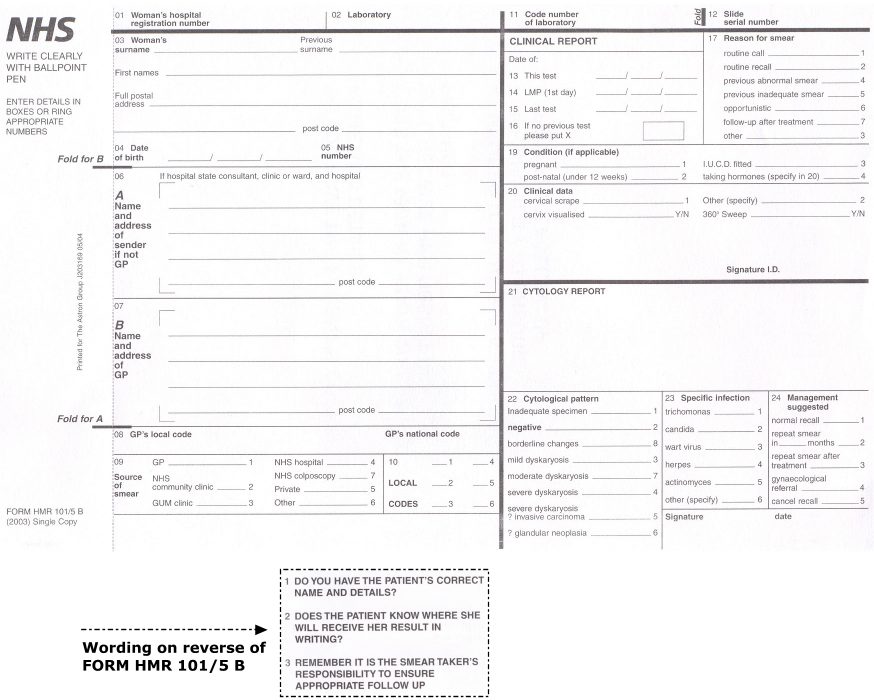
The national standard HMR101 form has been updated. There are two main alterations to the form that will affect sample takers and cytology laboratories:
Box 17 'Reason for smear' has been enhanced to provide a comprehensive set of options. Sample takers are requested to complete this box in accordance with the definitions given below to facilitate detailed evaluation of the cervical screening programme. - Box 20 'Clinical data'has been enhanced to include the questions:
- Cervix visualised - Yes or No? and
- 360° sweep - Yes or No?
The answers to these questions will assist the laboratory in making an informed judgement about sample adequacy in accordance with NHSCSP publication no. 1 'Achievable standards, Benchmarks for reporting, and Criteria for evaluating cervical cytopathology' which states "The cervix must be visualized at the time the sample is taken and the full circumference of the cervix must be sampled." It is imperative that these questions are answered accurately otherwise the sample will be reported as inadequate by default.
There are also a number of minor amendments to the form; these are described in the guidance notes below. All amendments will be introduced with the first issue of the reprinted HMR101 forms in the spring of 2004.
HMR101/5C and HMR101/5D withdrawn
The range of HMR101 forms has been reduced. Plain-back forms are no longer available from the Department of Health. Printed-back forms in both single-part and multi-part formats will continue to be available from Astron - Tel. 0161 683 2376
Printed-back forms have been amended to replace instructions on 'taking a cervical smear' with the following prompts:
- DO YOU HAVE THE PATIENT'S CORRECT NAME AND DETAILS?
- DOES THE PATIENT KNOW WHERE SHE WILL RECEIVE HER RESULT IN WRITING?
- REMEMBER IT IS THE SMEAR TAKER'S RESPONSIBILITY TO ENSURE APPROPRIATE FOLLOW UP
Guidance Notes for Completion
The HMR101 form is used for cervical or vaginal smears. The majority of boxes 01 to 20 of the form are completed by the smear taker. The form is then sent with the cell sample to the laboratory. Smear takers should ensure that all information provided on the HMR101 form is complete and legible to support the laboratory in assessing the adequacy of the smear, producing an accurate report, making appropriate recommendations for future management of the woman and notifying the correct organisations of the smear result and next actions.
The laboratory will complete the form and make a report to the smear taker, the woman's GP (if different) and the administrator of the call/recall system for the cervical screening programme. If multi-part forms are used, the laboratory may send each colour-coded part to the appropriate organisation. If single-part forms are used, the laboratory will send printed or electronic reports directly from the laboratory computer system to each organisation.
Detailed instructions on each element of the form are given below. Note that these instructions refer to the national standard HMR101 form and not to locally designed variations which may be numbered or arranged differently or include alternative data fields and/or options.
| HMR101 Request/Report Form for Cervical or Vaginal Cytology |
|---|
| Box No. |
Information Required |
Usage Instructions |
| Box 01 |
Woman's hospital registration number |
Record the woman's locally-allocated hospital or unit number (if applicable). |
| Box 02 |
Laboratory |
Record the name or site of the laboratory which will be reporting the smear. |
| Box 03 |
Woman's surname
Previous surname
First names
Full postal address
Postcode |
Record the key demographic information of the woman to provide up-to-date contact details. This information is also necessary for patient identification and therefore allows the laboratory to link previous smear results with this test. |
| Box 04 |
Date of Birth |
Record the woman's actual date of birth to indicate her age and also to assist in patient identification and record linking. The woman's age will affect interpretation of the smear and is therefore significant. |
| Box 05 |
NHS number |
Record the woman's NHS number. This should be a 10-digit number displayed in a 3-3-4 format. This is required for patient identification and is particularly useful to support electronic data communications. |
| Box 06 |
Name and address of sender if not GP
(If hospital state consultant, clinic or ward, and hospital)
Postcode |
Record the name and address of the organisation where the smear taker is based (if this is not the woman's own GP practice) |
| Box 07 |
Name and address of GP
Postcode |
Record the name and address of the woman's GP. If the woman is not currently registered with a GP, this should be noted. |
| Box 08 |
GP's local code
GP's national code |
Record the local and national codes used to identify the woman's GP. The national code gives a unique organisation identifier. The local code is unique only within the local area and so one local code may be used for a different GP in another area. |
| Box 09 |
Source of smear:
1 = GP
2 = NHS Community Clinic
3 = GUM clinic
4 = NHS hospital
5 = Private
6 = Other
7 = NHS Colposcopy |
Indicate which type of organisation the smear taker is acting for at the time of this smear.
Code 1 (GP) is to be used for any smear taken by a direct employee of the GP practice, regardless of the location e.g. home visit. The smear taker may be the GP, a practice nurse or other qualified health professional.
Code 2 (community clinic) is to be used for smears taken at local NHS clinics e.g. family planning clinics.
Code 3 (GUM clinic) is to be used for smears taken at GUM or other sexual health clinics.
Code 4 (NHS hospital) is to be used for smears taken at hospital clinics such as maternity clinics. Smears taken under GUM, at colposcopy or where the woman is being treated/screened as a private patient are excluded. Also excluded are smears from GP or community clinics on hospital premises.
Code 5 (Private) is to be used for any smear from a private patient.
Code 6 (Other) is to be used for smears from sources which are not otherwise classifiable e.g. workplace or charitable screening services.
Code 7 (NHS colposcopy) is to be used for screening or follow-up smears taken at NHS colposcopy clinics.Note that only smears from source types 1 and 2 are classed as screening smears for the purposes of evaluation of the NHS Cervical Screening Programme. |
| Box 10 |
Local codes: (1 - 6) |
This box is to be used by local arrangement only. |
| Box 11 |
Code number of laboratory |
Record the laboratory identification code. |
| Box 12 |
Slide serial number |
Record the slide identification number. This information is required for record linkage and to facilitate audit. |
| CLINICAL REPORT |
| Box 13 |
Date of this test |
Record the date that the smear was taken from the woman. |
| Box 14 |
Date of LMP (1st day) |
Record the date that was the first day of the woman's last menstrual period. This information together with date of test is required for the laboratory to calculate the exact day of the menstrual cycle which influences the interpretation of the smear, particularly in older women. Date of LMP should therefore be given as accurately as possible .If the woman is amenorrheic (e.g. post-menopausal, pregnant, using Depo Provera), the best estimate (month and/or year) of the LMP should be given. This, together with consideration of the woman's age and hormonal status (see box 19), will also influence the interpretation of the smear. |
| Box 15 |
Date of last test |
Record the date of the woman's last smear test (if applicable and/or if known). |
| Box 16 |
If no previous test, put X in box |
Indicate if the woman has never had a smear test before, adequate or inadequate. Do not mark this box if there is uncertainty about the existence of a previous test. |
| Box 17 |
Reason for smear:
1 = routine call
2 = routine recall
4 = previous abnormal smear
5 = previous inadequate smear
6 = opportunistic
7 = follow-up after treatment
3 = other |
Indicate the reason for the smear test, selecting one option only. This information will be used for detailed evaluation of the NHS Cervical Screening Programme from 2003.
Code 1 (routine call) is to be used for women responding to an invitation for routine screening who have never before had an adequate smear, regardless of the number of previous invitations. See note 1 below.
Code 2 (routine recall) is to be used for women responding to an invitation for routine rescreening. The woman's last attended test is likely to have been coded 'A' (routine recall) for next action. See note 1 below.
Code 4 (previous abnormal smear) is to be used where a woman is undergoing repeat screening due to a previous borderline or mildly abnormal result which was coded 'R' (early repeat) for action. This abnormal result may have been some months or years earlier and may have been followed by one or more subsequent negative tests. However, until the woman is returned to routine recall, code 4 should continue to be used. Code 4 may also be used for next smears from women who were referred for colposcopy due to one or more abnormal smears (any degree of abnormality) but who did not attend.
Code 5 (previous inadequate smear) is to be used where a woman's previous smear result was inadequate (result code '1') and the reason for the previous test was not known. Otherwise a repeat smear for a previous inadequate should be coded according to the original reason for the smear. Code 5 should also be used for:- smears from women referred for colposcopy following a series of inadequate tests- next smears from women referred for colposcopy following a series of inadequate tests but who did not attend.
Code 6 (opportunistic) is to be used for smears from women who are eligible for routine call/recall (i.e. no previous test or no recent test which was abnormal) but who are not responding to a formal invitation for screening. This may include women who are tested while ceased from the programme e.g. those who have opted out. See note 1 below.
Code 7 (follow-up after treatment) is to be used where a woman requires cytological surveillance after a colposcopy attendance regardless of whether or not the colposcopy resulted in biopsy/treatment. Cytological surveillance is usually indicated by the 'R' (early repeat) action code. If a woman is returned to routine recall after negative colposcopy (action code 'A'), code 7 should not be used for subsequent smears.
Code 3 (other) is to be used for smears which do not fit into any other category, for example smears taken at first visit to colposcopy.
Note 1
An invitation is defined as a written letter notifying a woman that her smear test is due. The screening service, the GP practice or the laboratory may send invitations. A woman attending for screening within six months of the date of invitation is considered to be responding to that invitation. Attendance's more than six months after a routine invitation should be classed as opportunistic (code 6). Attendance's at any time after an early repeat invitation should be classed according to the reason for the repeat e.g. previous abnormal (code 4) or follow-up (code 7).
If the date and/or type of the woman's most recent invitation are not known and cannot be estimated based on her known screening history, it is acceptable to assume that the smear is opportunistic (code 6). |
| Box 18 |
Not used |
Data items from box 18 have been relocated to box 20. |
| Box 19 |
Condition (if applicable):
1 = pregnant
2 = post-natal (under 12 weeks)
3 = I.U.C.D.fitted
4 = taking hormones (specify in 20) |
Indicate which (if any) of the options are applicable and provide details where necessary in box 20. This information is required by the laboratory as the woman's hormonal status influences interpretation of the smear. |
| Box 20 |
Clinical data
1 = Cervical scrape
2 = Other (specify)__________
Cervix visualised Y / N
360° sweep Y / N |
Indicate the type of specimen.
For cervical smears, state if the cervix was visible during the examination and if the full circumference of the cervix was sampled. This will enable the laboratory to determine the adequacy of the smear.
Provide all information relating to current signs and symptoms. Also provide brief details of any significant history including abnormal cytology (with slide number) and previous diagnosis and treatment. This will ensure that the laboratory has sufficient information to make an appropriate recommendation on future management of the woman.
|
Signature
ID: | Sign and provide smear taker identification code (by local agreement only). |
| Box 21 |
CYTOLOGY REPORT |
Provide a full report using free text or standard report codes according to local practice. |
| Box 22 |
Cytological pattern:
1 = inadequate specimen
2 = negative
8 = borderline changes
3 = mild dyskaryosis
7 = moderate dyskaryosis
4 = severe dyskaryosis
5 = severe dyskaryosis/
?invasive carcinoma
6 = ?glandular neoplasia |
Indicate the cytological pattern of the sample, selecting one option only. |
| Box 23 |
Specific infection:
1 = trichomonas
2 = candida
3 = wart virus
4 = herpes
5 = actinomyces
6 = other (specify) |
Indicate which, if any, infections are present in the sample (by local agreement only). |
| Box 24 |
Management suggested:
1 = normal recall
2 = repeat smear in __ months
3 = repeat smear after treatment
4 = gynaecological referral
5 = cancel recall |
Indicate the next recommended action, selecting one option only.
Code 1 (normal recall) is to be used for all cases where the next test is due at the routine recall interval which may be up to 54 months. This corresponds to action code 'A'.
Code 2 (repeat in 'm' months) is to be used where the next test is due at an early or fixed interval. This corresponds to action code 'R'.
Code 3 (repeat after treatment) is to be used where, for example, the smear cannot be reported due to infection. This corresponds to action code 'R'.
Code 4 (gynaecological referral) is to be used where the woman requires a referral for colposcopy or where she has been referred and is to remain under the colposcopist's care pending return to call/recall. This corresponds to action code 'S'.
Code 5 (cancel recall) is no longer used. The laboratory may not remove a woman from call/recall. If code 5 is selected it is treated in the same way as code 1. Note that a woman whose next test would become due after age 65 will be removed from call/recall automatically provided that there are no indications to the contrary, for example a recent abnormal screening result.
|
| |
Signature
Date |
Sign and give the date that the smear was reported. |
Please send all queries to [email protected]
Frequently Asked Questions
Q1. Why has the number of options for 'reason for smear' been extended?
A1. Previously there were four categories of reason for smear; this was insufficient for all scenarios. The new comprehensive set of categories provides an option for every situation. This will allow more accurate provision of data that will in turn facilitate better evaluation of the cervical screening programme.
Q2. What is the 'reason for smear' for smears taken at colposcopy?
A2. This will depend upon the reason for referral:
If an abnormal smear (any degree of abnormality) - use code 4 (previous abnormal smear)
If an inadequate smear - use code 5 (previous inadequate smear)
If a negative smear or no smear - use code 3 (other)
Q3. What is the 'reason for smear' if the woman had a mild or borderline smear several years ago but her most recent test result was negative?
A3. This will depend upon the woman's status:
If the woman is still under surveillance (last test coded 'R' for action) - use code 4 (previous abnormal smear)
If the woman has been returned to routine recall - use code 2 (routine recall)
Q4. If I do not specify that the cervix was visualised and/or confirm the 360° sweep, will the smear be reported as inadequate automatically?
A4. The laboratory will examine the sample and if there are any abnormalities present these will be reported otherwise it is likely that the smear will be classed as inadequate.
|
Cervical screening programme index
What happens at a
screening appointment?
Cervical cancer
Diethylstilbestrol (DES) exposed women
Liquid Based Cytology (LBC)
LBC implementation guidance
Who does what in the NHS Cervical Screening Programme
Frequently Asked Questions (FAQs)
Quality assurance
Programme statistics
Archived statistics bulletins
Cytology training
Human Papilloma Virus (HPV)
HPV Sentinel Sites
HMR 101 guidance notes
Research
Useful links
Publications
Programme posters
Archive
|